



Quick Study Analysis: Is Autism Increasing Or Not?
tl;dr: Is the apparent increase just measurement error? Moments like this are why I am such a skeptic of those who claim to be authorities...

“Autism rates increased 60-fold in 30 years, not because of vaccines or environmental toxins, but because of changes in the way autism is defined.”

Is The Increase In Autism Measurement Error?
Prof. Gøtzsche is one of the leading advocates of evidence-based medicine, and a vehement critic of the pharmaceutical industry. He was one of the founders of the Cochrane Collaboration, and wrote the book Deadly Medicines and Organised Crime: How Big Pharma Has Corrupted Healthcare.

I generally agree with his positions. In this case, I was a bit surprised to see this post. While I’m skeptical of many aspects of psychology, is it really plausible that the explosion in autism cases is entirely an artifact of definition?
He’s linking to this NY Times editorial: “Autism Rates Have Increased 60-Fold. I Played a Role in That.”
“Allen Frances is a psychiatrist. He led the American Psychiatric Association’s task force charged with creating the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders.” (Frances, 2025)
The DSM is basically a manual and definition of psychiatric illnesses. When you go see a shrink, they’re going to take an inventory of your symptoms, and put you in a bucket (a disease) defined by the DSM.
I think I like Dr. Frances.
“In preparing the DSM-IV, we attempted to hold the line against diagnostic inflation and the medicalization of normality; however, we failed.” (Frances, 2014)
He explains that they expanded the diagnosis of autism to include Asperger’s, and they expected this to slightly increase the rate of diagnoses of autism-related conditions.
“Based on careful studies, our task force predicted that the addition of Asperger’s syndrome would modestly increase the rate of children given an autism-related diagnosis. Instead, the rate increased more than 16-fold, to one in 150 from an estimated one in 2,500 in the span of a decade. It has been climbing more gradually ever since and is one in 31 today.” (Frances, 2025)
The Claim
Then he makes a claim:
“The role, if any, of environmental toxins is still to be determined, but there is no known environmental factor that can explain the sudden jump in diagnoses. The changes we made to the diagnosis in the D.S.M.-IV can.” (Frances, 2025)
That sounds like the implementation of the Dietary Guidelines. Designed to reduce obesity (among other things) its creation was accompanied by a dog-leg upwards in obesity incidence.

Was their such a change in the data after the DSM-IV was introduced in 1994?
The Data
My first attempt to find some decent data was not entirely fruitful, but interesting.
“Factors known to account for the rise in prevalence include the increase in community awareness and public health response globally, changes in case definition that have broadened diagnostic boundaries over time, increased diagnosis of milder forms, and increase in the identification of autism in previously under‐diagnosed populations defined by sex, geography, race/ethnicity, or SES. To date, there is weak or conflicting evidence for the hypothesis that geographic variation or time trends in prevalence may reflect differences in exposure to environmental risk factors (Nevison, 2014) or increased patterns of migration (Keen et al., 2010).” (Ziedan, 2022)

They also point out that “case definition” has played a role in the increased prevalence, and find a far-larger-than-60-fold difference between different populations. Compare Australia and Canada, for instance, two populations of similar genetic extraction that have far different rates.
“Two main clinical references are most frequently used to determine autism ‘caseness’: the Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association and the International Classification of Diseases (ICD) of the World Health Organization (WHO); the most recent editions are the ICD-11 (First et al., 2015) and the DSM-5 (American Psychiatric Association, 2013). The DSM-5 is already in use whereas the ICD-11 will come into use in 2022.” (Ziedan, 2022)
The ICD definition of autism follows the DSM, so there is effectively one world-wide definition, however problematic it may be.
Unfortunately they don’t get into the changes in time in autism diagnoses. They note they are increasing in some areas, stable in others. The increases are still happening ~20 years after the DSM-IV was released, although that may reflect further changes to the definition in the current DSM (DSM-5).
Here's a better dataset.

There's no inflection point around the release of DSM IV. The increase started long before it was released. They used the California dataset because it is the oldest, and one can see that there is a long, steady increase in autism rates, and then an inflection up around 1980.
Hmm…
The found a similar pattern in other states. The increase started long before DSM-IV, and there’s no obvious inflection at that point.

In an earlier paper from the same author, she looked directly at Frances’ claim.
“Before embarking on the trend analysis of the suspected environmental compounds, the temporal trend in autism itself is examined.… A new, empirical approach is applied to test the hypothesis that autism is a constant-prevalence condition that simply has been underdiagnosed in the past.” (Nevison, 2014)
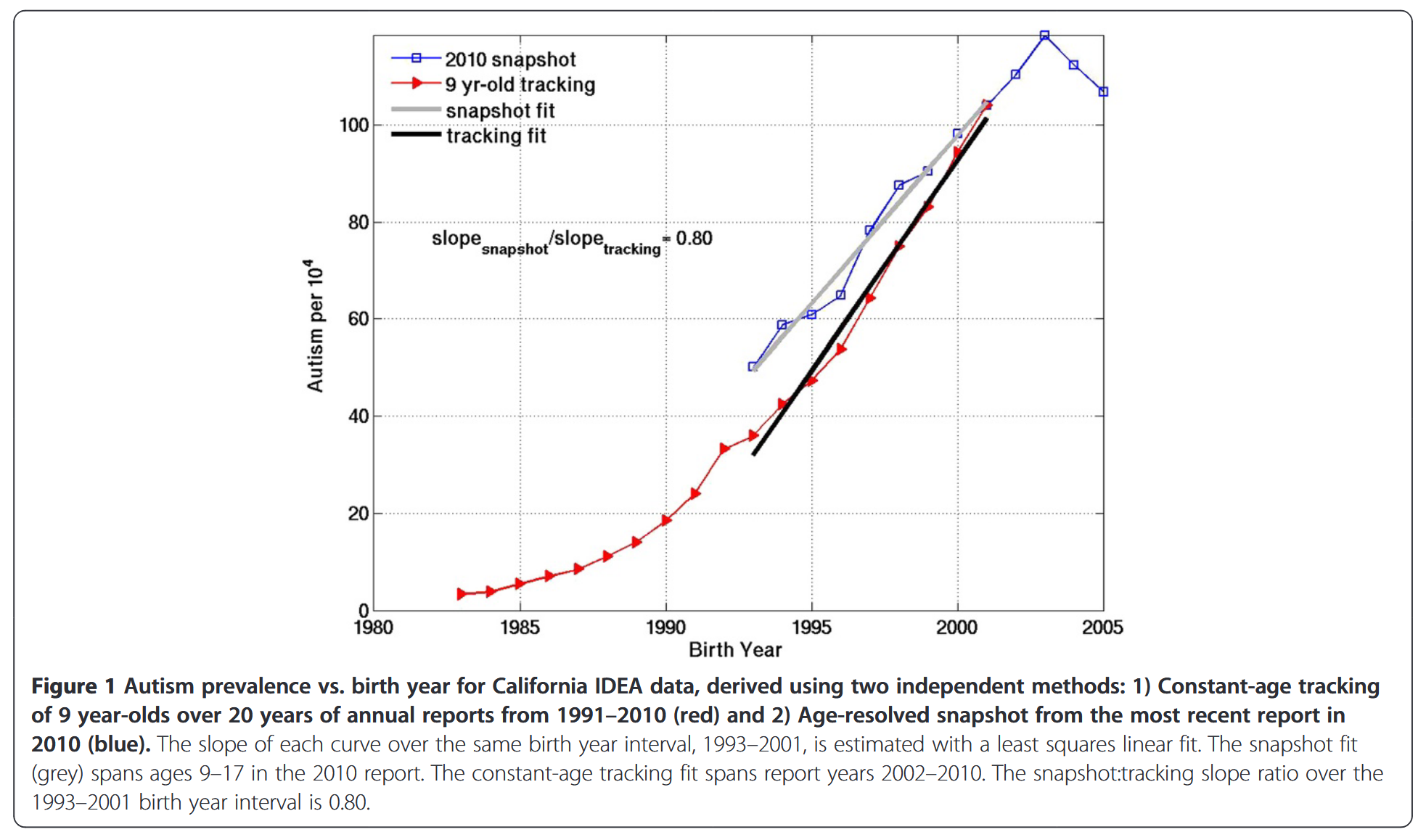
Obviously the finding is the same. What’s interesting is the quantification.
“Results—Temporal trend in U.S. autism” The slope ratios for the California IDEA age-resolved snapshot and constant-age tracking trends suggest that about 80% of the tracked increase in California autism is “real” as opposed to due to better diagnosis, both for birth year intervals 1988 to 1994–1997 and 1993 to 1999–2002 (Figure 1).” (Nevison, 2014)
So the change in diagnosis seems to have an effect, but it’s not even a majority of the effect. Again, it’s clear that the increase was under way well before DSM-IV in 1994.
Environmental Factors
This paper looks at a number of putative environmental triggers for autism. I’m going to ignore the factors that decreased, as they can’t account for the continued increase. This includes thimerosol, and total blood mercury, by the way. From (Nevison, 2014):
Trends increasing
Polybrominated diphenyl ethers (PBDEs)
Cumulative aluminum adjuvants
Cumulative total immunizations
Glyphosate
Maternal obesity
You’ll notice what’s missing from the “environmental factors” list: any diet items. Obesity gets closest.
Glyphosate is pretty interesting.

Again, like with the DSM-IV change in diagnosis, it follows the increase, it does not precede it. Glyphosate was introduced in 1974, but didn’t enter widespread use until the 1990s.
“Based purely on these timing considerations, it appears that glyphosate cannot be responsible for the first autism cases in the 1930s and is unlikely to have caused the late 1980s uptick, but could be interacting in recent years with other toxins to drive up the prevalence of U.S. autism.” (Nevison, 2014)
Glyphosate is of course used to produce seed oil crops, like soy.
Maternal obesity is getting more to the point. Here the increase is contemporaneous to the increase in obesity, at that magical 1980 timepoint.

“Notably, Additional file 1: Figure S21 shows that the time trend in obesity among U.S. women correlates well to that of autism, suggesting maternal obesity may be a direct influence or a comorbid consequence of the dietary factors contributing to autism, or both.” (Nevison, 2014)
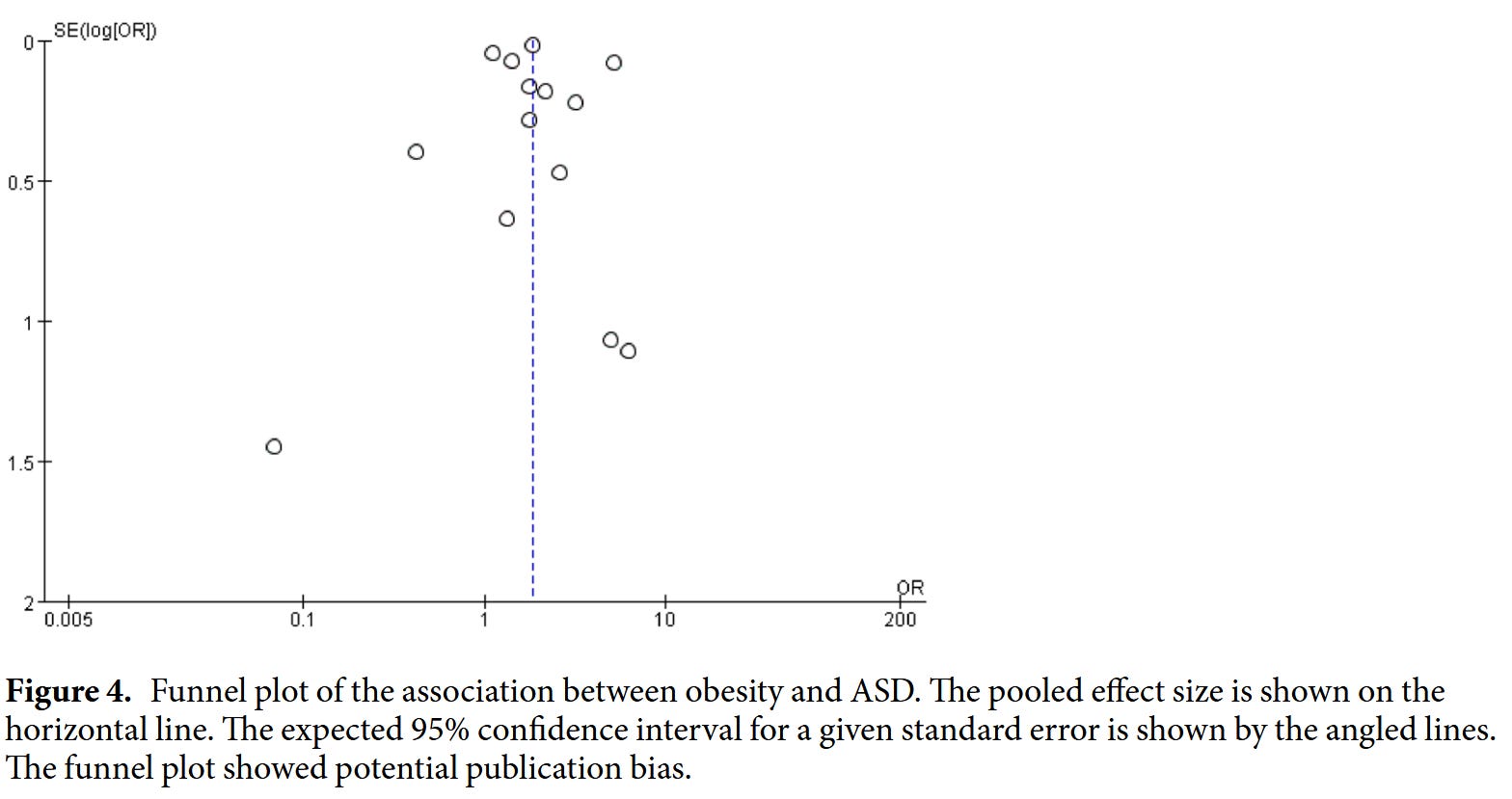
While this is news to me, it’s well-enough known in the literature that there’s a meta-analysis looking at the relationship:
“This meta-analysis included 15 studies with a total of 49,937,078 participants and 1,045,538 cases of ASD [autism spectrum disorder—the DSM-5 term]. The results showed that obesity but not overweight was associated with ASD.” (Zheng, 2017)
Conclusion
I think it’s clear that Frances is getting ahead of himself by taking credit for the increase in autism. It’s clear that it long predates his role in the DSM-IV, and the release of the new standard.
Gøtzsche should have done a little bit of work to find out if Frances’ claim was credible before making that post on X, and Frances should clearly have done so. Why didn’t the Times’ fact-checkers notice what I noticed immediately? To ask that question is to answer it—the Times is not concerned with facts.
Regardless of the individual or the esteem they are held in, it’s always a good idea to double-check a claim, especially when it seems too good or unlikely.
Honestly, I hadn’t even considered the role of obesity for this post. When I included the Dietary Guidelines graph, I was simply looking for an example of a trend that dog-legged up, without having to create one myself!
Once I noticed that the dog-legs were the same, however…
I have another autism post planned, based on another study I found recently, that may shed some light on how autism and obesity may be related.
References
Frances, Allen. “Autism Rates Have Increased 60-Fold. I Played a Role in That.” The New York Times, June 23, 2025, sec. A. https://www.nytimes.com/2025/06/23/opinion/why-autism-rates-increased.html?unlocked_article_code=1.RE8.IbSb.EKbVfMXEA8mj&smid=nytcore-android-share
Frances, Allen. “DSM, Psychotherapy, Counseling and the Medicalization of Mental Illness: A Commentary from Allen Frances.” The Professional Counselor 4, no. 3 (July 2014): 282–84. https://doi.org/10.15241/afm.4.3.282.
Gøtzsche, Peter C. “Autism Rates Increased 60-Fold in 30 Years, Not Because of Vaccines or Environmental Toxins, but Because of Changes in the Way Autism Is Defined. Https://Bit.Ly/46aMT7K. @brokenmedics, @SecKennedy, @martinkulldorff, @StabellBenn, @DrJBhattacharya, @MartyMakary, @cdcgov, @WHO Https://T.Co/LAb7LcEhq0.” Tweet. Twitter, June 25, 2025. https://x.com/PGtzsche1/status/1937718630235480451.
Nevison, Cynthia D. “A Comparison of Temporal Trends in United States Autism Prevalence to Trends in Suspected Environmental Factors.” Environmental Health 13, no. 1 (September 5, 2014): 73. https://doi.org/10.1186/1476-069X-13-73.
Nevison, Cynthia, Mark Blaxill, and Walter Zahorodny. “California Autism Prevalence Trends from 1931 to 2014 and Comparison to National ASD Data from IDEA and ADDM.” Journal of Autism and Developmental Disorders 48, no. 12 (December 1, 2018): 4103–17. https://doi.org/10.1007/s10803-018-3670-2.
Zeidan, Jinan, Eric Fombonne, Julie Scorah, Alaa Ibrahim, Maureen S. Durkin, Shekhar Saxena, Afiqah Yusuf, Andy Shih, and Mayada Elsabbagh. “Global Prevalence of Autism: A Systematic Review Update.” Autism Research 15, no. 5 (2022): 778–90. https://doi.org/10.1002/aur.2696.
Ah-huh.
Just ask any adult older than 50 how many autistic kids they knew when they were growing up. And compare that to the numbers that are in our schools now.
Where did they used to hide them all?
And if there were as many then as now, where are all the autistic adults who were those children? I'm not talking about the quirky ones who give TED talks and write on social media. I'm talking about the ones who cannot function in independent living settings, who shuffle around with noise-canceling headphones eating only chicken nuggets and French fries. Who cannot toilet themselves or hold a job without outside support.
Peter Bowtie talks like a shill for pharma.
Also, if the increase is due strictly to broadened diagnostic criteria, why is the increase continuing? Seems that once the previously unidentified folks are now identified (surely it's been long enough!), the increase would plateau.
I just finished reading *Neurotribes* which makes this same argument (that autism rates spiked because of DSM reclassification). But that book came out in 2016. The longer time series correlations we have, the more these types of arguments weaken. (Though these correlations were available to the author; it would be interesting to see if they continue to hold in the intervening 15 years.)