



How Mitochondrial Defects Can Cause Various Seemingly Unrelated Diseases
tl;dr: Anyone who has dealt with electrical problems will understand this issue.

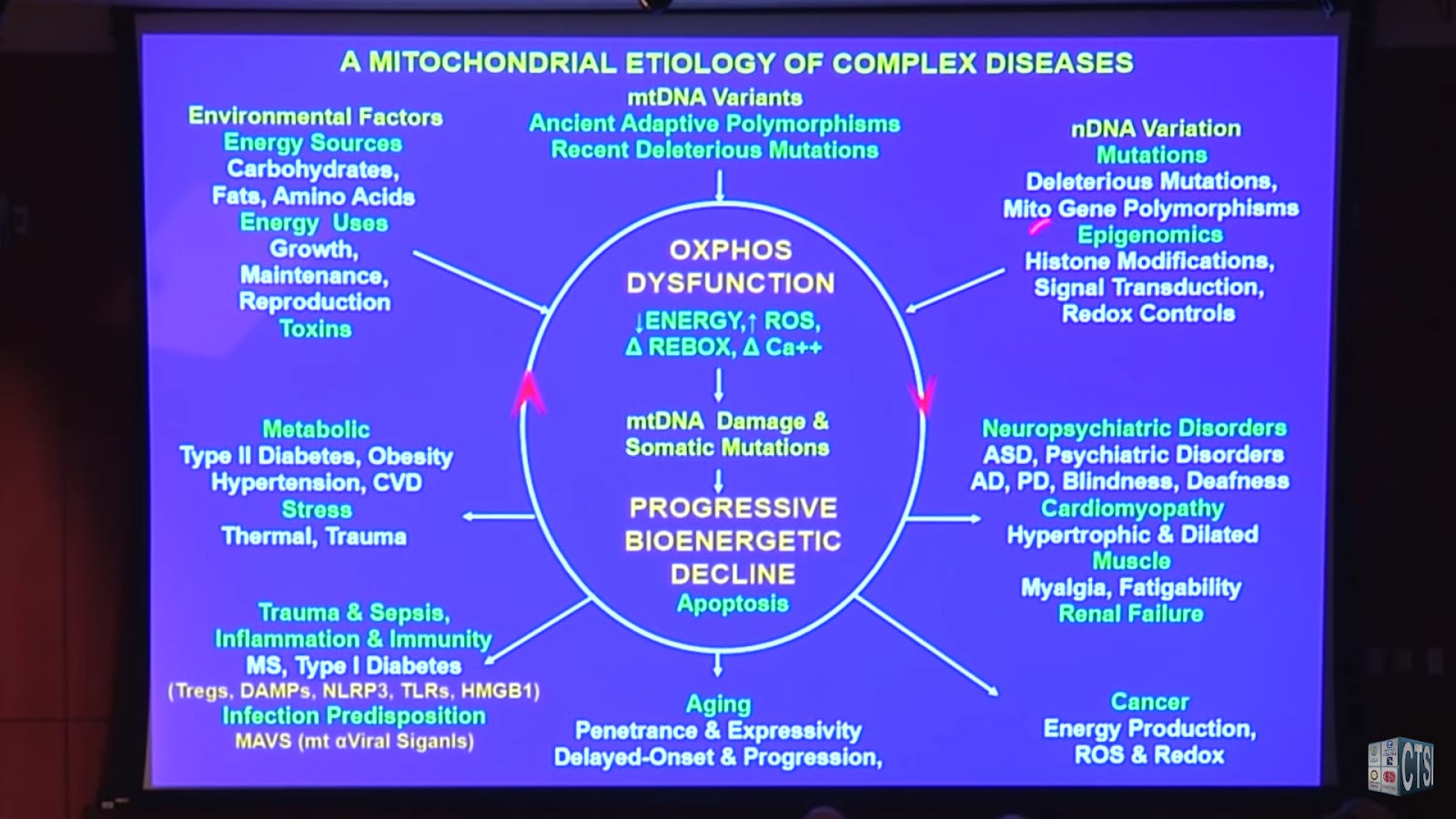
"A Mitochondrial Etiology of Common Complex Diseases" [1]
An hour-long discussion of how mitochondrial dysfunction can result in various chronic diseases, and how the assumption that an anatomical division of disease is a driving assumption for how medicine is organized, and how that may block correct description and diagnosis of disease.
The speaker is Douglas C. Wallace, Ph.D.; Director, Center for Mitochondrial and Epigenomic Medicine (CMEM); Professor, Department of Pathology & Laboratory Medicine, The Children's Hospital of Philadelphia.
He does an especially good job of describing how malfunction in a single organelle can cause various diseases in various seemingly unrelated organs.
Some useful quotes below the video:
"Our hypothesis (that we've been testing for the last 45 years) is that bioenergetic dysfunction lies at the nexus of the genetic and environmental "causes"; and that the "common-complex" diseases are bioenergetic diseases, and not anatomical diseases." 7:07.
"Now each cell has hundreds of thousands of these mitochondrial DNAs, and they're constantly replicating inside your cells right now. And if you doubt that they're active and vital in there, talking to each other; tonight when it's very very quiet and your spouse is not snoring if you just concentrate you'll feel them wiggling in there." 16:49
Discussing cells with different mitochondrial genotypes from mutation and division:
"Some with good mitochondrial DNAs and high energy, some with bad mitochondrial DNAs and low energy, and if it's below the minimum energy for that tissue, then you will get a phenotype. The equivalent of a biological, a metropolitan brownout. So if there was a line voltage decline in LA, all the electrical systems wouldn't fail at one time. The first thing that would go would be the fluorescent light bulbs, then certain elevators, then certain electrical motors, but the incandescent light bulbs would just get dimmer and dimmer.
"Well the same is true for your body. Different parts of your body rely on energy to different extents, so as the energy declines, you're going to get organ-specific symptoms of a systemic defect." 17:35
Noting the wild variation in expression between mitochondrial defects:
"If you inherit that from your mother you're fine until midlife, and then you'll lose your hearing (sensory-neural hearing loss). But if you get treated by aminoglycoside antibiotics, you'll go deaf within a week. OK? Mutation in the tRNA leucine gene, another protein synthesis mutation at 3243; at 30 % mutant will give you diabetes, 50% mutant give your neuromuscular disease, 100% mutant and you are dead." 18:55
He goes on with many more examples.
"So we have a quantitative genetics with totally different clinical phenotypes." 20:15'

Tissue-specific Symptomatology
"So why would there be tissue-specific symptomatology? Well because different tissues rely on mitochondrial energy for different extents [sic]... [Examples] ...So in fact when you think energetically, much of anatomy is about energetics, not anatomy." 21:12
"The take-home lesson"
"If the, in fact, the cells are sick, they cannot undergo apoptosis, then the mitochondria are released into the bloodstream, and they are perfectly good bacteria, and you're going to get inflammation. And that's why we believe all of these diseases have an inflammatory component." 23:54
He doesn't discuss my favorite topic, the impact of omega-6 fats on mitochondria and therefore health, but it fits nicely with his hypothesis. For instance, the part of mitochondria that causes the immune reaction and inflammation he describes is cardiolipin released with oxidized linoleic acid into the blood stream. [2]
Do watch the whole thing!
References
1. A Mitochondrial Etiology of Common Complex Diseases. UCLA CTSI; 2017. https://www.youtube.com/watch?v=1aCHrHwm_AI. Accessed December 20, 2019.
2. Tuominen Anu, Miller Yury I., Hansen Lotte F., Kesäniemi Y. Antero, Witztum Joseph L., Hörkkö Sohvi. A Natural Antibody to Oxidized Cardiolipin Binds to Oxidized Low-Density Lipoprotein, Apoptotic Cells, and Atherosclerotic Lesions. Arteriosclerosis, Thrombosis, and Vascular Biology. 2006;26(9):2096-2102. doi:10.1161/01.ATV.0000233333.07991.4a
Having watched the whole thing, I kept wondering when Dr. Wallace was going to say something of this sort. "The degree of fatty acid unsaturation of mitochondrial membrane lipids has been found to be one of those biochemical parameters that are most strongly correlated with longevity, when different species of mammals and birds are compared, with a low degree of fatty unsaturation being correlated with less lipid peroxidation and a longer normal life-span." https://lipidworld.biomedcentral.com/articles/10.1186/1476-511X-9-37
I did an 'adipose arachidonic acid mitochondrial function' web search. The AI (artficial intelligence) Overview that came up ahead of the articles said, "Arachidonic acid (AA) in adipose tissue can negatively impact mitochondrial function, potentially contributing to metabolic disorders like obesity and type 2 diabetes. Specifically, AA can increase reactive oxygen species (ROS) production, reduce respiratory capacity, and affect mitochondrial membrane potential, ultimately leading to reduced energy production and overall mitochondrial dysfunction."
An 'adipose arachidonic acid mitochondrial function' web search brought up an AI Overview that said, "Linoleic acid (LA), an essential fatty acid, plays a crucial role in adipose tissue and mitochondrial function, particularly in brown adipose tissue (BAT). Linoleic acid is a major component of cardiolipin (CL), a phospholipid in the inner mitochondrial membrane, which is vital for mitochondrial membrane structure and function. A diet rich in linoleic acid can lead to enhanced mitochondrial uncoupling and improved oxidative phosphorylation (OXPHOS) in BAT, contributing to metabolic benefits like decreased adiposity and improved insulin sensitivity."
That's why epidemiologists draw this conclusion. "Using large prospective datasets, higher blood levels of LA were associated with lower risk of coronary heart disease, stroke and incident type-2 diabetes mellitus compared with lower levels, suggesting that, across the range of typical dietary intakes, higher LA is beneficial. Recent trials of LA-rich oils report favorable outcomes in people with common lipid disorders." https://lipidworld.biomedcentral.com/articles/10.1186/s12944-024-02246-2
Norwegian animal science researchers explain how that works. "Because AA competes with EPA and DHA as well as with LA, ALA and oleic acid for incorporation in membrane lipids at the same positions, all these fatty acids are important for controlling the AA concentration in membrane lipids, which in turn determines how much AA can be liberated and become available for prostaglandin biosynthesis following phospholipase activation. Thus, the best strategy for dampening prostanoid overproduction in disease situations would be to reduce the intake of AA, or reduce the intake of AA at the same time as the total intake of competing fatty acids (including oleic acid) is enhanced, rather than enhancing intakes of EPA and DHA only." https://lipidworld.biomedcentral.com/articles/10.1186/1476-511X-9-37
It is important to note that only people who already have lipid disorders will experience improvement in insulin sensitivity with increased linoleic acid intake. The same sort of improvement can be induced with oleic acid with far less risk.
What the Norwegians recommend is bascally a Mediterranean style dietary approach which looks like this. "The Mediterranean diet is low in arachidonic acid and rich in healthy fats such as monounsaturated fats found in extra-virgin olive oil (EVOO), nuts and omega-3 fatty acids from fish, which has been shown to lower the risk of inflammation, heart disease, cancer, diabetes and obesity, and other degenerative diseases." https://advancedmolecularlabs.com/blogs/news/new-red-meat-study-controversy